
Ectopic Pregnancy
Overview
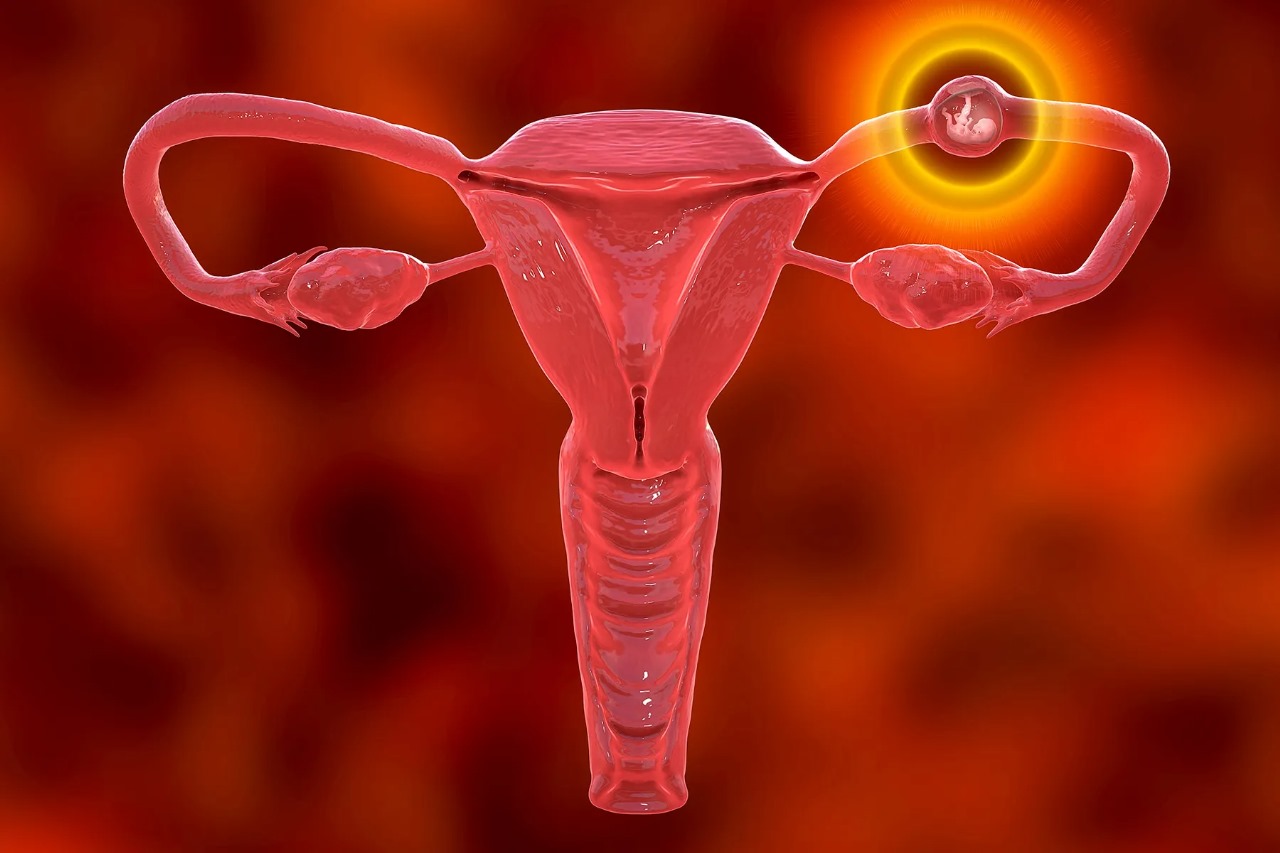
An ectopic pregnancy is defined as the implantation of a fertilized ovum outside the endometrial lining of the uterine cavity, most commonly within the ampullary portion of the fallopian tube. This condition poses a significant risk of tubal rupture and life threatening intra-abdominal hemorrhage, and therefore constitutes a gynecological emergency requiring timely recognition and management.
For Advanced Gynecological Surgery, we are committed to early diagnosis and comprehensive management of ectopic pregnancies, with an emphasis on minimally invasive techniques, fertility preservation, and patient safety.
Clinical Presentation
Clinical Presentation
The symptomatology of ectopic pregnancy can be variable. Common clinical features include:
• Lower abdominal or pelvic pain
• Amenorrhea followed by vaginal spotting or bleeding
• Shoulder tip pain, suggestive of diaphragmatic irritation from intraperitoneal bleeding
• Dizziness, syncope, or signs of hypovolemic shock in the event of rupture
Not all patients exhibit the classic triad of pain, amenorrhea, and bleeding. A high index of suspicion is essential for early detection.
Etiology and Risk Factors
Ectopic implantation results from impaired tubal motility or structural damage to the fallopian tube. Identified risk factors include:
• Prior ectopic pregnancy
• Tubal surgery or tubal pathology, including pelvic inflammatory disease (PID)
• Use of assisted reproductive technologies (ART) such as IVF
• Intrauterine device (IUD) in situ at conception
• Cigarette smoking
• Congenital or acquired tubal anomalies
Importantly, up to 50% of ectopic pregnancies occur in women with no identifiable risk factors.
Diagnostic Approach
Diagnosis is based on a combination of clinical, laboratory, and imaging modalities:
1. Clinical Evaluation
Detailed history and physical (especially pelvic) examination to assess tenderness, adnexal mass, or cervical motion tenderness.
2. Serial Quantitative β-hCG
In viable intrauterine pregnancies, β-hCG typically doubles every 48–72 hours. Plateauing or suboptimal rise suggests an abnormal pregnancy.
3. Transvaginal Sonography (TVS)
The primary imaging modality. Findings may include:
o Absence of intrauterine gestational sac despite elevated β-hCG
o Presence of adnexal mass or free fluid in the pouch of Douglas
4. Additional Investigations
o CBC to evaluate anemia
o Blood group and Rh typing
Management Strategies
Treatment is individualized based on:
• Hemodynamic stability
• β-hCG levels
• Sonographic findings
• Patient’s reproductive desires
1. Expectant Management
• Considered in selected asymptomatic patients with low and declining β-hCG levels and no evidence of rupture.
• Requires close surveillance with serial β-hCG and ultrasound.
2. Medical Management
• Indicated in hemodynamically stable patients with unruptured ectopic pregnancy and no contraindications.
• Single or multi-dose protocols may be used, with post-treatment β-hCG monitoring until resolution.
• Advantages: Tubal preservation, avoidance of surgery.
3. Surgical Management
• Indicated for:
o Suspected or confirmed tubal rupture
o Hemodynamic compromise
o High or rising β-hCG levels
o Failure of medical therapy
• Laparoscopic surgery is the preferred approach:
o Salpingostomy – Removal of ectopic tissue with tubal conservation (when feasible)
o Salpingectomy – Removal of the affected tube (when tubal integrity is compromised)
Specializing in advanced laparoscopic and robotic-assisted gynecologic surgery, delivering optimal patient outcomes through:
• Reduced postoperative pain
• Shorter hospital stays
• Lower complication rates
• Enhanced fertility preservation when clinically appropriate