
Ovarian Cyst Management
Overview
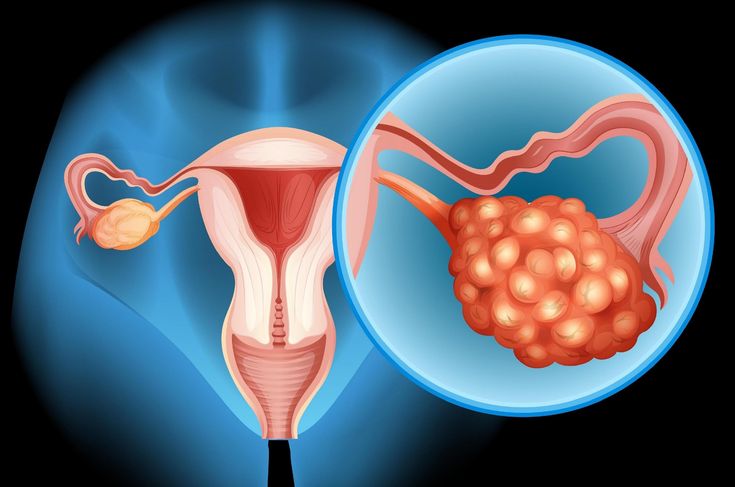
Ovarian cysts are fluid-filled sacs arising from the ovarian tissue. While the majority are functional and benign, resolving spontaneously, some cysts may cause complications such as rupture or ovarian torsion. These complications necessitate prompt diagnosis and intervention to prevent morbidity.
Pathophysiology and Clinical Significance
• Ruptured Ovarian Cyst: The rupture leads to spillage of cystic fluid into the peritoneal cavity, potentially causing peritoneal irritation, acute abdomen, hemoperitoneum, and significant pelvic pain. Internal hemorrhage may result depending on the cyst type and vascular involvement.
• Ovarian Torsion: This occurs when an enlarged ovary – often due to a cyst – twists around the suspensory ligaments, resulting in compromised arterial inflow and venous outflow. The ensuing ischemia poses a risk of ovarian necrosis, requiring emergent surgical detorsion to preserve ovarian viability.
Clinical Presentation
Patients with ovarian cyst complications may present with:
• Sudden onset of severe unilateral lower abdominal or pelvic pain
• Associated nausea and vomiting
• Abdominal distension or bloating
• Syncope or presyncope
• Dyspareunia or dyschezia
• Menstrual irregularities
Diagnostic Workup
Accurate diagnosis relies on a multimodal approach:
• Transvaginal and/or Transabdominal Ultrasonography: Initial imaging modality to characterize cyst morphology, size, and presence of free fluid.
• Doppler Ultrasonography: Critical for assessing ovarian vascular perfusion and detecting torsion.
• Cross-sectional Imaging (CT/MRI): Employed selectively for equivocal cases or complex adnexal masses.
• Laboratory Investigations: CBC to assess for anemia or infection, inflammatory markers, and pregnancy testing to exclude ectopic pregnancy.
● Tumour markers: to rule out ovarian malignancies
Management Strategies
1. Conservative Management
• Indicated for asymptomatic, small, simple cysts.
• Management includes analgesia, observation, and serial imaging to monitor resolution.
2. Surgical Intervention
• Indicated for symptomatic, large, complex cysts, ovarian torsion, or ruptured cysts with significant bleeding.
• Minimally Invasive Techniques: Laparoscopic cystectomy or detorsion is preferred due to reduced morbidity, preservation of ovarian tissue, and faster recovery.
• Robotic-assisted Surgery: Offers enhanced precision in complex cases.
3. Emergency Surgery
• Indicated in hemodynamically unstable patients or when ischemic ovarian damage is suspected.
• Goals include control of hemorrhage, cyst excision, and ovarian salvage if viable; otherwise, oophorectomy may be necessary.
Postoperative Care and Surveillance
• Routine postoperative follow-up with pelvic ultrasonography to assess ovarian recovery and exclude recurrence.
• Hormonal and fertility evaluation as indicated.
• Patient education on symptom recognition and preventive strategies.
When to Seek Urgent Care
Presentation with acute, severe lower abdominal pain, accompanied by systemic symptoms such as syncope or vomiting, mandates immediate medical evaluation to rule out ovarian torsion or cyst rupture and to initiate timely management.